Overview

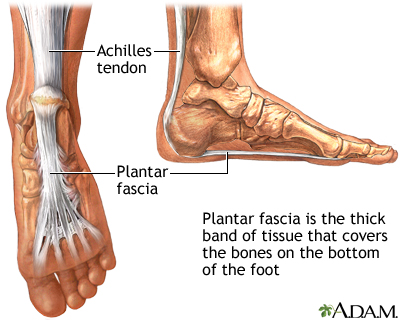
The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape. At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed.
bestshoelifts
Non Surgical Treatment
The type of treatment will depend on the stage of PTTD present. There are four stages of posterior tibial tendon dysfunction. Stage I. The posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. The patient can still perform a single-limb heel rise and has a flexible hindfoot. Orthotic treatment options include modified off the shelf inserts and custom molded orthotics. Stage 2. The tendon is partially torn or shows degenerative changes and as a result loses strength.There is considerable flattening of the arch without arthritic changes in the foot. The patient cannot perform single-limb heel rise. Pain is now present on the lateral aspect of the ankle. Orthotic treatment is similar as that in stage I, with the addition of more rigid arch supports and wedging. Stage 3. Results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. A solid ankle AFO is suggested in conjunction with a modified orthopedic shoe. Stage 4. Is identical to stage three except that the ankle joint also becomes arthritic. A rigid AFO and modified orthopedic shoe is required.
Surgical Treatment

Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.
The human foot is a complex structure that absorbs shock every time we take a step. The foot has to adapt to a variety of movements during different forms of activities such as walking, running and climbing steps. The foot is made up of many different joints, ligaments and muscles which have to work together to allow us to move and balance. The arch of the foot plays and important role in absorbing shock and preventing over stressing of the foot muscles and bones. In this article, we shall briefly discuss flat feet and fallen arches. These two conditions are closely related to each other and can increase the risk of overuse injury to the foot. They can also cause overload of more proximal structures such as ankles, shins, knees and the lower back.
Causes
There are many different causes of flat feet, which can be separated into two main categories. The first category, congenital flat foot, is a condition that one is born with or is predisposed to at birth. This type includes the completely asymptomatic, pediatric flexible flat foot-by far the most common form of congenital flat foot. Flexible means that an arch is present until weight is put on the foot, at which time the arch disappears. This foot type is a result of the fact that all people are born with different physical features. Some people have bigger noses than others, just as some people have flatter feet (of course, there is no known correlation between the two). Any alteration in the many building blocks of the foot can influence its shape. At the other end of the spectrum, yet within the same category of congenital flat foot, exist several rare, more severe forms of flat foot. These severe conditions include Vertical Talus, Congenital Calcaneal Valgus, and Tarsal Coalitions - all of which are more rigid (no arch with or without weight on the foot) and definitely symptomatic. Luckily, these are much less common, but can usually be identified by specialists at the time of presentation and treated appropriately. The second category, acquired flat foot, develops over time, rather than at birth. Many different factors can contribute to the development of flat feet. These include the types of shoes a child wears, a child's sitting or sleeping positions, compensation for other abnormalities further up the leg, or more severe factors such as rupture of ligaments or tendons in the foot. Very commonly, the reason for flat feet is that the foot is compensating for a tight Achilles tendon. If the Achilles tendon is tight, then it causes the foot to point down, or to plantarflex (as occurs when stepping on the accelerator of your car). Even minimal amounts of plantarflexion can simulate a longer leg on that particular side, assuming that the other foot is in the normal position. The body therefore tries to compensate by pronating, or flattening out the arch, thereby making up for the perceived extra length on the affected side.
Symptoms
Flat feet may not cause any symptoms at all. Rigid flat feet may cause pain, calluses, blisters, or skin redness on the inner side of the foot. A stiff foot, weakness or numbness of the foot, Rapid wearing out of shoes-worn shoes lean in toward each other. Difficulty or pain with activities like running-in the foot, knee or hip.
Diagnosis
Most children and adults with flatfeet do not need to see a physician for diagnosis or treatment. However, it is a good idea to see a doctor if the feet tire easily or are painful after standing, it is difficult to move the foot around or stand on the toes, the foot aches, especially in the heel or arch, and there is swelling on the inner side of the foot, the pain interferes with activity or the person has been diagnosed with rheumatoid arthritis. Most flatfeet are diagnosed during physical examination. During the exam, the foot may be wetted and the patient asked to stand on a piece of paper. An outline of the entire foot will indicate a flattened arch. Also, when looking at the feet from behind, the ankle and heel may appear to lean inward (pronation). The patient may be asked to walk so the doctor can see how much the arch flattens during walking. The doctor may also examine the patient's shoes for signs of uneven wear, ask questions about a family history of flatfeet, and inquire about known neurological or muscular diseases. Imaging tests may be used to help in the diagnosis. If there is pain or the arch does not appear when the foot is flexed, x-rays are taken to determine the cause. If tarsal coalition is suspected, computed tomography (CT scan) may be performed, and if an injury to the tendons is suspected, magnetic resonance imaging (MRI scan) may be performed.
bestshoelifts
Non Surgical Treatment
The type of treatment will depend on the stage of PTTD present. There are four stages of posterior tibial tendon dysfunction. Stage I. The posterior tibial tendon is inflamed but has normal strength. There is little to no change in the arch of the foot. The patient can still perform a single-limb heel rise and has a flexible hindfoot. Orthotic treatment options include modified off the shelf inserts and custom molded orthotics. Stage 2. The tendon is partially torn or shows degenerative changes and as a result loses strength.There is considerable flattening of the arch without arthritic changes in the foot. The patient cannot perform single-limb heel rise. Pain is now present on the lateral aspect of the ankle. Orthotic treatment is similar as that in stage I, with the addition of more rigid arch supports and wedging. Stage 3. Results when the posterior tibial tendon is torn and not functioning. As a result the arch is completely collapsed with arthritic changes in the foot. A solid ankle AFO is suggested in conjunction with a modified orthopedic shoe. Stage 4. Is identical to stage three except that the ankle joint also becomes arthritic. A rigid AFO and modified orthopedic shoe is required.
Surgical Treatment
Surgery for flat feet is separated into three kinds: soft tissue procedures, bone cuts, and bone fusions. Depending on the severity of the flat foot, a person?s age, and whether or not the foot is stiff determines just how the foot can be fixed. In most cases a combination of procedures are performed. With flexible flat feet, surgery is geared at maintaining the motion of the foot and recreating the arch. Commonly this may involve tendon repairs along the inside of the foot to reinforce the main tendon that lifts the arch. When the bone collapse is significant, bone procedures are included to physically rebuild the arch, and realign the heel. The presence of bunions with flat feet is often contributing to the collapse and in most situations requires correction. With rigid flat feet, surgery is focused on restoring the shape of the foot through procedures that eliminate motion. In this case, motion does not exist pre-operatively, so realigning the foot is of utmost importance. The exception, are rigid flat feet due to tarsal coalition (fused segment of bone) in the back of the foot where freeing the blockage can restore function.
After Care
Time off work depends on the type of work as well as the surgical procedures performed. . A patient will be required to be non-weight bearing in a cast or splint and use crutches for four to twelve weeks. Usually a patient can return to work in one to two weeks if they are able to work while seated. If a person's job requires standing and walking, return to work may take several weeks. Complete recovery may take six months to a full year. Complications can occur as with all surgeries, but are minimized by strictly following your surgeon's post-operative instructions. The main complications include infection, bone that is slow to heal or does not heal, progression or reoccurrence of deformity, a stiff foot, and the need for further surgery. Many of the above complications can be avoided by only putting weight on the operative foot when allowed by your surgeon.



 Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.
Morton?s Neuroma is a pain condition that affects your feet and toes. If you are suffering from Morton?s Neuroma, a growth of tissue has developed over one of the nerves running from your feet into your toes. This growth can cause inflammation and pain whenever you use your foot. A type of benign tumor, Morton?s Neuroma typically develops in the space between the third and fourth toes, although it can also form between the second and third toes. When you walk, the bones and ligaments in the top of your foot press down on this growth, causing pressure and pain.




 Overview
Overview Symptoms
Symptoms Prevention
Prevention Some people have massive bunions that aren?t that painful but cause difficulties with shoes, while others have relatively small bunions that are very painful. However, just because you have Hallux valgus doesn?t mean you?ll get the bursa. Pressure from the big toe joint can lead to a deformity in the joint of the second toe, pushing it toward the third toe and so on. Likewise, if the second toe and big toe cross over, it can be difficult to walk. Once the big toe leans toward the second toe, the tendons no longer pull the toe in a straight line, so the problem tends to get progressively worse. This condition can also encourage corns and calluses to develop.
Some people have massive bunions that aren?t that painful but cause difficulties with shoes, while others have relatively small bunions that are very painful. However, just because you have Hallux valgus doesn?t mean you?ll get the bursa. Pressure from the big toe joint can lead to a deformity in the joint of the second toe, pushing it toward the third toe and so on. Likewise, if the second toe and big toe cross over, it can be difficult to walk. Once the big toe leans toward the second toe, the tendons no longer pull the toe in a straight line, so the problem tends to get progressively worse. This condition can also encourage corns and calluses to develop.